
12 Revenue Cycle Management Mistakes Costing You Revenue
- Updated Date Feb 18, 2026
- Revenue Cycle Management
- Follow
Revenue loss in 2026 is rarely caused by one major failure. It is usually the result of small process gaps that repeat every day across the revenue cycle.
A fee schedule is not updated after a contract change. Eligibility is confirmed as active, but the deductible reset is missed. A prior authorization is approved, but the CPT code billed does not match the approval. A claim goes out with the wrong place of service. Each issue seems minor at the time. Over weeks and months, they reduce reimbursement, increase denials, and slow cash flow.
Most revenue cycle mistakes are not complex. They happen in routine tasks such as verification, coding, claim submission, follow-up, and payment posting. When workflows are rushed or inconsistently reviewed, small errors move downstream and become harder to correct.
This guide outlines the 12 most common and costly revenue cycle management mistakes providers are making today. These are practical issues that occur in real billing operations and directly affect reimbursement, denial rates, and accounts receivable performance.
What Is Revenue Cycle Management?
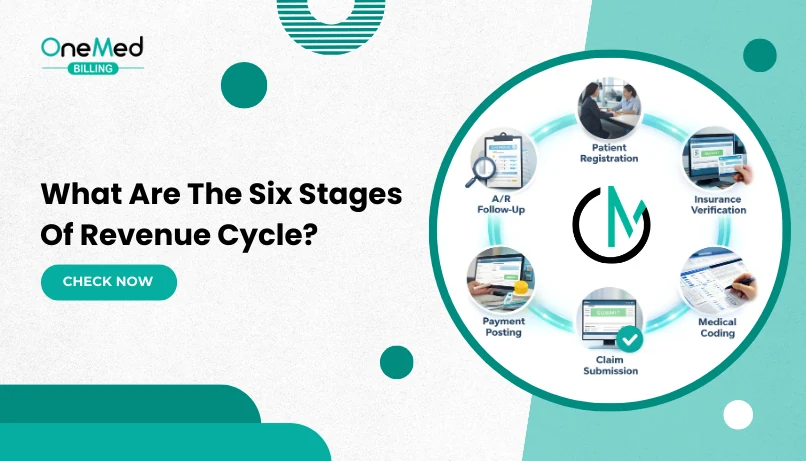
Revenue cycle management (RCM) is the process healthcare providers use to track patient care from appointment scheduling to final payment. It includes eligibility verification, coding, claim submission, payment posting, and patient collections. The goal is to ensure accurate billing and timely reimbursement while minimizing denials and revenue delays.
Revenue cycle management typically involves three stages:
1. Before Care (Pre-Service)
Patient information is collected and verified. Eligibility, benefits, referrals, and prior authorizations are confirmed. Cost estimates are provided, and copays or deposits are collected when applicable.
2. During Care (Point of Service)
Clinical documentation is completed accurately. Services are coded correctly using the appropriate diagnosis and procedure codes. Required modifiers are applied, and charges are captured.
3. After Care (Post-Service)
Claims are reviewed and submitted to the payer. Payments are posted through ERA and EFT. Denials are addressed, underpayments are identified, and remaining patient balances are billed and collected.
The 12 Most Costly Revenue Cycle Management Mistakes in 2026
Revenue cycle management mistakes in 2026 are less about major failures and more about repeated operational gaps. As payer automation increases and authorization, coding, and documentation rules tighten, small process errors now trigger faster denials and payment delays.
Workflows that are not consistently monitored create avoidable revenue leakage. Individually, these issues may seem minor. Collectively, they slow cash flow, increase rework, and raise administrative costs.
Below are the most costly revenue cycle management mistakes providers continue to make and why they persist.
Mistake 1: Outdated Fee Schedules and Contract Rates
This mistake happens when internal fee schedules or payer contract rates are not updated after reimbursement changes. Billing systems may still reflect last year’s pricing or outdated allowables. Payments post normally, but the reimbursement does not match the contracted amount. Because underpayments often appear as standard contractual adjustments, they go unnoticed. Over time, small discrepancies across high-volume CPT codes lead to steady revenue loss.
This typically happens when:
- Annual contract updates are not loaded into the billing system
- Fee schedules are updated but modifier differentials are not
- Site-of-service pricing differences are ignored
- Contract rate monitoring reports are not reviewed
- Underpayments are written off automatically without review
Mistake 2: Incomplete Insurance Eligibility Verification
Eligibility is often checked only for active coverage, not for full benefit details. Staff may skip deductible status, referral requirements, network tier placement, or coordination of benefits. Returning patients are sometimes not re-verified, especially at the start of a new plan year. These gaps result in claims applying to deductible, processing out-of-network, or denying for missing referrals. The issue begins at the front desk but surfaces weeks later during adjudication.
This typically happens when:
- Eligibility is verified days before the visit and not rechecked
- Only the “active” status is reviewed
- Secondary insurance is assumed instead of confirmed
- Referral requirements are not validated
- January deductible resets are not accounted for
Mistake 3: Poor Prior Authorization Oversight
Prior authorization errors occur when approvals do not align with what is ultimately billed. CPT codes may change after authorization, units may exceed limits, or services may be performed outside approved dates. In busy workflows, authorization status is assumed instead of confirmed. Because many payers apply automated authorization edits, mismatches often lead to full denials rather than partial reductions.
This typically happens when:
- Authorizations are requested after scheduling
- Clinical documentation is incomplete at submission
- CPT codes are updated but auth is not revised
- Units exceed what was approved
- Expiration dates are not tracked
Mistake 4: Missed Coding and ICD-10 Updates
Each year, diagnosis and procedure codes are revised, added, or deleted. When EHR systems and billing tools are not fully updated, outdated or invalid codes are submitted. Providers may also continue using unspecified diagnoses when greater detail is required. Clearinghouses and payers reject these claims automatically. Coding gaps slow payment and increase rework.
This typically happens when:
- ICD-10 updates are not fully implemented in the EHR
- Retired codes remain in provider favorites
- Providers rely on templates not updated annually
- Specificity requirements are overlooked
- Coding audits are infrequent
Mistake 5: Documentation That Does Not Support Medical Necessity
Clinical notes sometimes lack the specificity needed to justify the billed service. The diagnosis may not clearly support the procedure, or required details such as laterality or severity may be missing. When documentation does not align with payer coverage policies, claims deny for lack of medical necessity. The issue is not the service itself, but how it is documented.
This typically happens when:
- Diagnosis is listed without linking it to the service
- Required clinical indicators are missing
- Repeat services lack updated justification
- Documentation templates are too generic
- Providers assume medical necessity is obvious
Mistake 6: Modifier Errors on Common Services
Modifiers are frequently missed, misused, or incorrectly applied. This often happens with E/M services performed on the same day as procedures, telehealth visits, or services during global surgical periods. Without the correct modifier, payers bundle services or reduce payment. Because modifier rules vary by situation, small coding inconsistencies create recurring payment issues.
This typically happens when:
- E/M with procedure lacks modifier 25
- Modifier 59 is used incorrectly or omitted
- Telehealth POS and modifier combinations do not match
- Global period rules are overlooked
- Laterality modifiers are missing
Mistake 7: Incorrect Place of Service or Taxonomy
Place of service (POS) codes directly affect reimbursement. When POS does not match where care was delivered, reimbursement can change significantly. Similarly, if provider taxonomy does not align with payer enrollment records, claims may deny or reprice. These errors typically occur during charge entry and go unnoticed until payment posts incorrectly.
This typically happens when:
- POS defaults are not locked by location
- Telehealth POS rules are misunderstood
- Provider taxonomy was updated but not reflected in billing
- Claims are copied from prior encounters without review
- Enrollment records and billing data are misaligned
Mistake 8: No Structured Pre-Bill Claim Review
Claims are sometimes submitted without thorough validation. Required fields may be missing, diagnosis-to-procedure links may not align, or authorization numbers may be absent. Without structured pre-bill review, these errors move downstream to clearinghouses and payers. The result is higher rejection rates and slower first-pass claim acceptance.
This typically happens when:
- Claim scrubbing tools are underutilized
- Required fields are not enforced
- Payer-specific edits are not configured
- Staff rush to submit claims at day-end
- First-pass acceptance rate is not tracked
Mistake 9: Delayed Claim Follow-Up
After submission, claims may not be actively monitored. Status responses go unchecked, portal messages are missed, and documentation requests are not addressed promptly. As claims age, resolution becomes more difficult. Delayed follow-up increases days in accounts receivable and reduces recovery likelihood.
This typically happens when:
- No structured aging buckets exist
- 277 claim responses are not reviewed
- Portal messages are checked inconsistently
- High-dollar claims are not prioritized
- Follow-up ownership is unclear
Mistake 10: Working Denials Without Identifying Patterns
Denials are often addressed individually instead of being analyzed collectively. When denial trends are not grouped by reason code, provider, or CPT, recurring issues continue unchecked. The same documentation or coding mistakes repeat month after month. Without pattern recognition, systemic errors remain unresolved.
This typically happens when:
- Denials are worked by date instead of reason
- No denial dashboard exists
- Provider-specific trends are not reviewed
- Root causes are not documented
- Monthly denial review meetings are skipped
Mistake 11: Incomplete ERA and EFT Reconciliation
Payments are sometimes posted in totals without reviewing line-by-line ERA detail. Underpayments, offsets, and takebacks may go unnoticed. When EFT deposits are not reconciled precisely against remittance data, discrepancies remain unresolved. Over time, small posting inconsistencies distort revenue reporting.
This typically happens when:
- Payments are posted in bulk
- PLB adjustments are ignored
- Contract rates are not validated
- EFT totals are not matched daily
- Cash posting and reconciliation lack separation
Mistake 12: Weak Patient Financial Communication
Patient financial responsibility has increased, but financial workflows have not always evolved with it. Cost estimates may be unclear, statements confusing, and payment options limited. When patients do not understand what they owe or how to pay, balances age quickly. This increases patient A/R and collection risk.
This typically happens when:
- Cost estimates are not provided upfront
- Statements lack clear breakdowns
- Payment options are limited to mail or phone
- Reminder cycles are inconsistent
- Staff struggle to explain insurance EOBs
How to Prevent Revenue Cycle Management Mistakes?
Preventing revenue cycle management mistakes requires structured oversight at every stage of the workflow. Errors rarely occur because teams lack effort, they occur when processes are inconsistent, responsibilities are unclear, or monitoring systems are weak.
The most effective prevention strategies focus on standardization, visibility, accountability, and continuous review.
1. Standardize Front-End Verification Processes
Front-end controls set the financial foundation for the entire encounter. Eligibility, benefits, referrals, and prior authorizations must be verified using consistent checklists rather than individual judgment. Verification should include deductible status, network validation, referral requirements, and coordination of benefits not just active coverage.
When front-end processes are standardized and documented, preventable denials and patient balance issues decrease significantly.
2. Maintain Updated Coding and Contract Data
Revenue integrity depends on accurate code sets and current payer contract terms. Annual ICD-10 and CPT updates must be fully implemented across EHR templates, billing systems, and claim scrubbers. Payer fee schedules and modifier adjustments should be reviewed regularly to ensure reimbursement aligns with contracted rates.
Failure to maintain updated data creates silent revenue loss through underpayments and avoidable rejections.
3. Implement Structured Claim Review Controls
Claims should pass through a consistent validation process before submission. This includes confirming required identifiers, diagnosis-to-procedure alignment, authorization numbers, modifier accuracy, and place-of-service consistency.
Structured pre-bill review improves first-pass claim acceptance rates and reduces downstream administrative rework. Preventing errors before submission is significantly more efficient than correcting them after denial.
4. Monitor Key Revenue Cycle Metrics Weekly
Performance visibility is essential. Organizations should track first-pass claim rate, denial rate, days in accounts receivable, underpayment trends, and patient A/R aging on a routine basis. Reviewing these metrics weekly not quarterly, allows teams to identify emerging issues before they escalate.
Consistent monitoring transforms revenue cycle management from reactive problem-solving into proactive performance management.
5. Analyze Denials by Root Cause
Denial management should focus on trend identification rather than isolated correction. Grouping denials by reason code, provider, payer, and CPT code helps identify recurring workflow gaps. When patterns are identified, process changes can be implemented to prevent repetition.
Without root-cause analysis, organizations risk repeatedly fixing the same issues without resolving the underlying problem.
6. Strengthen Payment Reconciliation and Reporting
Accurate cash posting and reconciliation ensure that reimbursement matches expectations. ERA data should be reviewed at the line-item level, and EFT deposits should reconcile precisely with posted payments. Underpayments and offsets must be identified and tracked rather than absorbed as routine adjustments.
Strong reconciliation processes protect revenue integrity and provide clearer financial reporting for leadership.
When to Consider Outsourcing Revenue Cycle Management?
Some revenue cycle issues are not caused by poor processes, but by limited capacity and oversight. If denial rates remain high, accounts receivable continues to age, or contract underpayments go unchecked, internal teams may not have the bandwidth to maintain consistent control.
In these situations, many providers choose to outsource revenue cycle management and billing to gain structured monitoring, specialized expertise, and clearer performance reporting. The goal is not just claim submission, but improved cash flow stability and reduced operational strain.
Whether managed internally or externally, revenue cycle performance depends on disciplined oversight and measurable accountability.
Conclusion
Revenue cycle performance does not improve through large overhauls. It improves through disciplined execution of the basics. Most revenue leakage comes from routine tasks that are rushed, inconsistent, or loosely monitored.
Eligibility must be verified completely. Authorizations must align exactly with what is billed. Codes and modifiers must match documentation. Claims must be reviewed before submission. Payments must be reconciled accurately. These are not advanced strategies. They are operational controls.
Organizations that consistently monitor these fundamentals reduce denials, shorten accounts receivable cycles, and protect contracted reimbursement. Those that do not continue to lose revenue in small amounts that compound over time.
Start by identifying the highest-impact breakdown in your current workflow. Correct it. Measure the result. Then move to the next. Incremental control creates measurable financial stability.
If your internal team lacks the capacity to maintain this level of oversight, structured revenue cycle support may be necessary. What matters most is not who manages the revenue cycle. What matters is that it is managed deliberately, consistently, and with clear accountability.
Frequently Asked Questions
Find quick answers to common questions about this topic, explained simply and clearly.
What are the most common revenue cycle management mistakes?
The most common revenue cycle management mistakes include: Incorrect or incomplete patient registration Failure to verify insurance eligibility before visits Missing prior authorizations Medical coding
How do RCM mistakes lead to denied claims and lost revenue?
RCM mistakes lead to denied claims when incorrect information is submitted to payors. Errors such as wrong patient details, invalid insurance coverage, coding mistakes, missing modifiers, or lack of authorization trigger automatic claim rejections.
What mistakes cause slow cash flow in the revenue cycle?
Slow cash flow in the revenue cycle is usually caused by: Delayed claim submission High denial rates Poor denial follow-up Failure to collect patient balances Inaccurate charge entry
What are the top medical billing errors that harm the revenue cycle?
The top medical billing errors that harm the revenue cycle include: Incorrect CPT or ICD coding Missing or incorrect modifiers Billing the wrong payor Duplicate claim submission Missing docu