


HCC Coding Explained - Guide for Accurate Risk Adjustment in 2026
- Updated Date Apr 29, 2026
- Medical Coding
- Follow
Medical billing professionals and physicians working with insurance plans need a clear understanding of Hierarchical Condition Category coding, what the model does, why accurate coding matters, and what the compliance requirements are. This blog covers each of those areas in detail to give a clear and comprehensive understanding of HCC coding.
What is Hierarchical Condition Category (HCC) Coding?
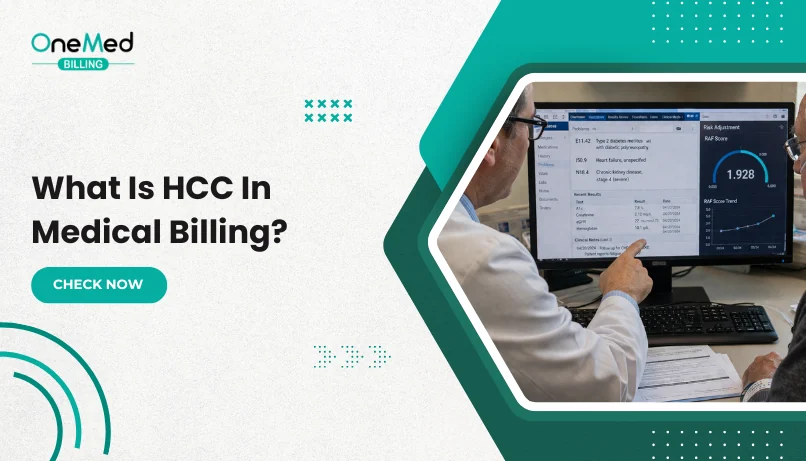
Hierarchical Condition Category coding, or HCC coding, is a risk adjustment model used by the Centers for Medicare & Medicaid Services (CMS) to estimate how medically complex a patient is likely to be in the coming year. That estimate determines how much CMS pays the health plan responsible for covering that patient.
The term "hierarchical" refers to how the model groups related conditions. When a patient has multiple diagnoses within the same clinical category, only the most severe one contributes to the risk calculation. For example, if a patient has both diabetes and diabetic polyneuropathy, the model uses only the more serious condition rather than counting both independently.
HCC coding applies primarily to Medicare Advantage plans, which are privately administered alternatives to traditional Medicare. These plans receive a fixed monthly payment per patient, and that payment is adjusted up or down based on the documented complexity of each patient's conditions. This is the mechanism risk adjustment is designed to serve.
The diagnosis codes that feed into the HCC model come from ICD-10. Not every ICD-10 code maps to an HCC. The model is built around chronic, serious, and high-cost conditions. Type 2 diabetes, congestive heart failure, chronic kidney disease, COPD, and morbid obesity are examples of conditions with HCC assignments. Acute or self-resolving conditions such as a respiratory infection or a minor injury do not map to HCCs.
Why is HCC Coding Important?
Here's the thing. A lot of practices don't take HCC coding as seriously as they should, and it ends up costing them real money without them even realizing it.
When HCC codes are captured accurately and completely, the health plan gets paid appropriately for the complexity of its patients. That payment then flows down to the practice in the form of better capitation rates and shared savings. When the coding is incomplete or vague, the plan gets paid less, and the practice suffers for it even though the patients are just as sick. Many practices solve this by working with a dedicated medical coding team that ensures all conditions are captured accurately.
Beyond the money, there's also the quality of care angle. Accurate HCC coding gives a clearer picture of what a patient is actually dealing with. It supports better care coordination, better chronic disease management, and better outcomes over time. So it's not just a billing thing. It's a patient care thing too.
And then there's compliance. CMS audits Medicare Advantage plans regularly. If codes are being submitted without proper documentation to back them up, that's a problem. Practices can face recoupments, audits, and worse if the coding doesn't match what's in the chart.
What Kinds of Conditions Do HCCs Represent?
Not every diagnosis is going to move the needle on risk adjustment. HCCs are specifically for conditions that are chronic, clinically significant, and likely to drive higher healthcare costs.
Some common examples include:
- Type 2 diabetes with and without complications
- Congestive heart failure
- Chronic kidney disease at various stages
- COPD
- Morbid obesity
- Diabetic polyneuropathy
- Vascular disease
- Major depression and other mental health conditions
- Cancer diagnoses
What doesn't usually map to an HCC is anything acute, minor, or self-resolving. The model is designed to capture the ongoing burden of illness, not one-off events.
One thing a lot of practices miss is the specificity piece. It's not enough to just say a patient has diabetes. You need to code it to the right level. Diabetes with diabetic polyneuropathy is a completely different HCC than diabetes with no complications, and it carries a much higher risk score. That difference in specificity translates directly into dollars.
How Does HCC Coding Affect Risk Adjustment and Value-Based Payment?
This is probably the most important section to understand, so let's take it slow.
Every Medicare Advantage patient gets a Risk Adjustment Factor (RAF) score. That score is built from a combination of demographic information like age and gender, and the HCC codes that have been documented and submitted for that patient. The higher the RAF score, the sicker the patient is considered to be, and the more the health plan gets paid to care for them.
The RAF score calculation adds up the weight of each qualifying HCC. Some conditions carry more weight than others depending on how expensive they are to manage. And because the model is hierarchical, if two conditions are related, only the more severe one gets counted.
This is why coding specificity matters so much. A patient coded at a lower level of severity will have a lower RAF score than they should. That means the plan is being underpaid, the practice may not be getting their fair share of capitation, and the patient's true clinical complexity isn't being captured anywhere.
In value-based care arrangements, this really shows up. Practices in shared savings programs, ACOs, or capitated contracts need accurate RAF scores to get credit for how complex their patient population actually is. If the scores are artificially low because of vague or incomplete coding, the practice is essentially leaving money on the table every single month.
Example 1: A 68-Year-Old Female with Type 2 Diabetes, Hypertension, and BMI of 38.2
Let's say this patient comes in for her annual wellness visit. Her chart documents type 2 diabetes with no complications, hypertension, and a BMI of 38.2 which puts her in the obese category. These conditions map to their respective HCCs and generate a modest RAF score. She's got chronic conditions but they're relatively well controlled and not highly complex. Her capitation payment reflects that.
Example 2: Same Patient with Diabetic Polyneuropathy, Morbid Obesity, and Congestive Heart Failure
Now let's say this same patient actually has diabetic polyneuropathy, her obesity is documented as morbid obesity with a BMI over 40 (even though the chart initially said 38.2), and she also has congestive heart failure. All of a sudden the RAF score looks very different. Each of those conditions maps to a higher-weight HCC. The capitation payment for this patient goes up significantly because she's genuinely more complex and more costly to care for. The coding did its job.
How Does HCC Coding Impact Billing and Reimbursement?
A lot of billing teams focus almost entirely on fee-for-service billing and think of HCC coding as someone else's problem. That's a mistake, especially as more practices move into value-based contracts.
In a Medicare Advantage context, accurate HCC coding affects how much the plan gets paid in capitation. And if your practice has a risk-sharing arrangement with that plan, your revenue is directly tied to how well your RAF scores reflect your patient population.
Undercoding is the big issue here. If a patient has three chronic conditions and only one of them gets coded, the RAF score is lower than it should be. The practice doesn't get credit for the full complexity of that patient. Over a panel of hundreds or thousands of Medicare Advantage patients, those gaps add up to a significant revenue shortfall.
Overcoding is the other side of it, and that's where compliance risk comes in. If conditions are being coded without documentation to support them, that's going to be a problem in an audit. Every HCC that goes on a claim needs to be supported by a physician note from that calendar year. CMS is strict about this, and so are the plans.
Example 1: Evolving HCC Models: Navigating the Transition from Version 24 to Version 28
For a long time, CMS used what's called HCC Version 24 as its standard risk adjustment model. But in recent years, CMS has been phasing in a new model called Version 28, and it changes quite a few things.
The transition didn't happen overnight. CMS used a blended approach through 2024 and 2025, meaning payment calculations were based partly on V24 and partly on V28. By 2026, V28 is expected to be fully implemented.
What is CMS-HCC V28 and What Does It Mean for Your Practice?
V28 is a significant update. It added a lot of new HCC categories, retired some older ones, and recalibrated the weights across the board. The goal was to make the model more accurate and more reflective of current clinical practice and healthcare costs.
Some conditions that carried a significant risk weight under V24 carry less weight under V28. Others got new categories or higher specificity requirements. This means practices that were doing reasonably well under V24 may see changes in their RAF scores under V28 even if their patient population hasn't changed.
The practical implication is that practices need to review their coding and documentation practices now. Conditions that were adequately coded under V24 might need to be documented with more specificity to capture the right category under V28. Coders need to be trained on the new mappings, and physicians need to understand why documentation specificity matters more than ever.
The transition to V28 is also hitting at the same time as other CMS changes, including upcoming RxHCC model updates expected in 2027. Staying ahead of these changes is not optional for practices that want to protect their revenue in value-based contracts.
Z Codes and Other Types of Risk Adjustment
Something that doesn't get talked about enough is how Z codes fit into the HCC picture. Z codes are ICD-10 codes used to capture things like social determinants of health, history of certain conditions, and status codes. They don't always map directly to HCCs, but they can support the clinical picture and fill in gaps in documentation.
For example, a Z code documenting a patient's housing instability or food insecurity doesn't directly affect the RAF score, but it adds context to the clinical record and supports the case for more intensive care management. Some Z codes do interact with HCC coding in specific ways, so coders should be familiar with when and how to use them.
Beyond HCCs, there are also RxHCC models which are used for the Medicare Part D drug benefit. These models use similar logic but are focused on predicting drug costs rather than overall medical costs. As CMS updates these models in 2027, practices and plans need to prepare in parallel with the HCC V28 transition.
Team-Based Strategies to Improve HCC Risk Adjustment
One of the most practical things a practice can do is stop treating HCC coding as a coding department problem and start treating it as a whole team problem.
The physician is the one who documents. The coder is the one who translates that documentation into codes. The biller makes sure those codes get submitted correctly. If any one of those people drops the ball, the HCC doesn't get captured.
Here are some strategies that actually work in practice:
1. Annual wellness visits are gold. This is the best opportunity to review and document all active chronic conditions. Every Medicare Advantage patient should be getting one, and the visit should include a full review of the problem list.
2. Chronic care management programs help keep conditions documented throughout the year, not just at annual visits. This is important because HCCs need to be supported by documentation from the current calendar year.
3. Regular coder and physician communication makes a big difference. Coders should be empowered to send queries back to physicians when documentation doesn't support the specificity needed for the right HCC. Physicians need to understand that those queries are about protecting revenue and accuracy, not about creating extra work.
4. Ongoing coder education is non-negotiable. HCC coding is not something you learn once and forget. With V28 now in play and more changes coming, coders need regular training on updated mappings and documentation requirements.
Key Reminders for HCC Coding Accuracy
Before wrapping up, here are the things that practices get wrong most often and what to do about them:
Code every year. HCCs don't carry over automatically. If a patient has diabetes, it needs to be documented and coded every single calendar year. One year of missed coding means that condition doesn't exist in the risk model for that year.
1. Code to the highest specificity
Unspecified codes are your enemy in HCC coding. Diabetes with complications is not the same as diabetes without complications. Morbid obesity is not the same as obesity. Every level of specificity matters.
2. Document what you treat
If a physician is managing a condition, it needs to be in the note. A condition that's being treated but not documented might as well not exist from a coding standpoint.
3. Support every code with documentation
This is the compliance piece. Every HCC submitted needs a physician note from that year that clearly supports the diagnosis. No documentation, no code.
4. Audit regularly
Internal audits help catch gaps before CMS or a health plan does. A regular audit cycle, even a small one, can identify patterns in undercoding or documentation gaps and fix them before they become a bigger problem.
HCC coding is one of those areas where getting it right really pays off, in more ways than one. Practices that invest in understanding it, training their teams on it, and building it into their day to day workflows are the ones that come out ahead in value-based care. And as Medicare Advantage keeps growing, that's only going to matter more.
Frequently Asked Questions
Find quick answers to common questions about this topic, explained simply and clearly.
What does HCC mean in coding?
HCC stands for Hierarchical Condition Category. It is a risk adjustment model used mainly by Centers for Medicare & Medicaid Services (CMS). In simple terms, HCC coding groups related medical conditions into categories. These categ
What are the three types of HCC coding?
HCC coding is generally used across three main programs: CMS-HCC - Used for Medicare Advantage plans to adjust payments based on patient risk. HHS-HCC - Used under ACA marketplace
What is the purpose of HCC?
The main purpose of HCC is to adjust payments based on patient health risk. Patients with more serious or chronic conditions require more care. HCC ensures that healthcare providers and plans receive fair reimbursement for treating these pati
What is an example of HCC coding?
A common example is a patient with diabetes and complications. Instead of coding it as a simple condition, the diagnosis is captured with specific ICD-10 codes that map to an HCC category. This category reflects higher risk c