What Is MDM in Medical Coding? Protect E/M Revenue and Avoid Errors
- Updated Date May 27, 2026
- Medical Billing
- Follow
Many practices lose money on E/M visits without realizing it. Not because the provider did less work, but because the documentation does not clearly show the complexity of the decision-making behind the visit.
A stable chronic condition, a medication change, test review, worsening symptoms, or a risk-based treatment decision can all affect the correct E/M level. But if those details are not documented properly, the visit may be undercoded, overcoded, denied, or exposed during audit review.
Medical Decision Making, or MDM, helps connect the provider’s clinical work to the correct E/M code. This guide explains how MDM works, what the three MDM elements mean, how they affect E/M code selection, and where practices commonly lose accuracy in documentation and coding. This guide explains how MDM works, what the three MDM elements mean, how they affect E/M code selection, and where practices commonly lose accuracy in documentation and coding.
What Is MDM?
MDM stands for Medical Decision Making. In medical coding, it is used to measure the complexity of an E/M visit based on what the provider had to evaluate, review, and decide during the patient encounter.
MDM does not only look at the diagnosis name. It looks at the full decision-making involved in the visit, such as the problems addressed, the data reviewed or ordered, and the risk involved in the patient’s condition or treatment plan.
For example, a patient with stable hypertension may support a lower E/M level if the visit only involves routine follow-up. But if the same patient has worsening blood pressure, medication changes, lab review, and risk discussion, the MDM level may be higher because the clinical decision-making is more complex.
MDM matters because it directly affects E/M code selection. If the documentation does not clearly support the MDM level, the visit may be coded too low, coded too high, denied, or questioned during an audit.
Why MDM Matters in E/M Coding?
MDM matters because it directly affects which E/M code is selected for a patient visit. The higher or lower the documented decision-making complexity, the more it can influence whether the visit supports codes such as 99213, 99214, or 99215.
For practice owners, this is important because inaccurate MDM can affect both revenue and compliance. If the MDM level is documented lower than the work performed, the practice may lose reimbursement. If it is documented higher than the record supports, the claim may create audit risk.
Accurate MDM helps the billing and coding team choose the right E/M level, reduce coding errors, support medical necessity, and make sure the provider’s clinical work is properly reflected in the claim.
The 3 Elements of MDM
MDM is based on three elements that show how complex the visit was and how much clinical decision-making the provider performed.
The three elements of MDM are:
- Problems addressed during the visit
- Data reviewed or analyzed
- Risk involved in the patient’s condition or treatment
Coders look at all three elements before selecting the final MDM level. In most cases, at least two of the three elements must support the same level. This means one serious diagnosis alone does not automatically support a higher E/M code unless the documentation also supports the required data review or risk level.
1. Number and Complexity of Problems Addressed
This looks at the patient problems the provider actually evaluated, treated, or managed during the visit. A diagnosis listed in the chart does not count by itself unless the provider addressed it during that encounter.
For example, a stable chronic condition may support a lower MDM level. A worsening chronic illness, a new problem with uncertain outcome, or a condition that could become serious may support a higher level if the documentation clearly shows it.
2. Amount and Complexity of Data Reviewed and Analyzed
This looks at the information the provider reviewed, ordered, or interpreted to make a clinical decision. This may include lab results, imaging, outside records, test orders, or discussion with another provider.
For example, ordering basic labs may support one level of data review. Reviewing outside records, ordering multiple tests, and discussing the case with another provider may support a higher level when documented clearly.
3. Risk of Complications, Morbidity, or Mortality
This looks at the risk connected to the patient’s condition and the treatment decisions made during the visit. Risk may come from medication management, worsening symptoms, surgery decisions, hospitalization decisions, or social factors that affect care.
For example, adjusting a prescription medication, managing a condition with serious risk, or considering hospitalization may increase the risk level when the provider documents the reason for that decision.
How MDM Levels Are Determined?
MDM levels are determined by reviewing three elements together: the problems addressed during the visit, the data reviewed or analyzed, and the risk involved in the patient’s condition or treatment plan.
Each element is assigned one of four levels:
- Straightforward
- Low
- Moderate
- High
To select the final MDM level, at least two of the three elements must meet or support the same level. A single high-level element does not automatically make the entire visit high complexity if the other two elements are lower.
For example, if the problem addressed is moderate, but the data reviewed and risk are both low, the overall MDM level will usually be low. To support a moderate MDM level, at least two elements must support moderate complexity.
This is why coders should not choose an E/M level based on diagnosis alone, data alone, or risk alone. Accurate MDM coding requires reviewing the full encounter and confirming that the documentation supports the selected level.
How MDM Levels Affect E/M Code Selection?
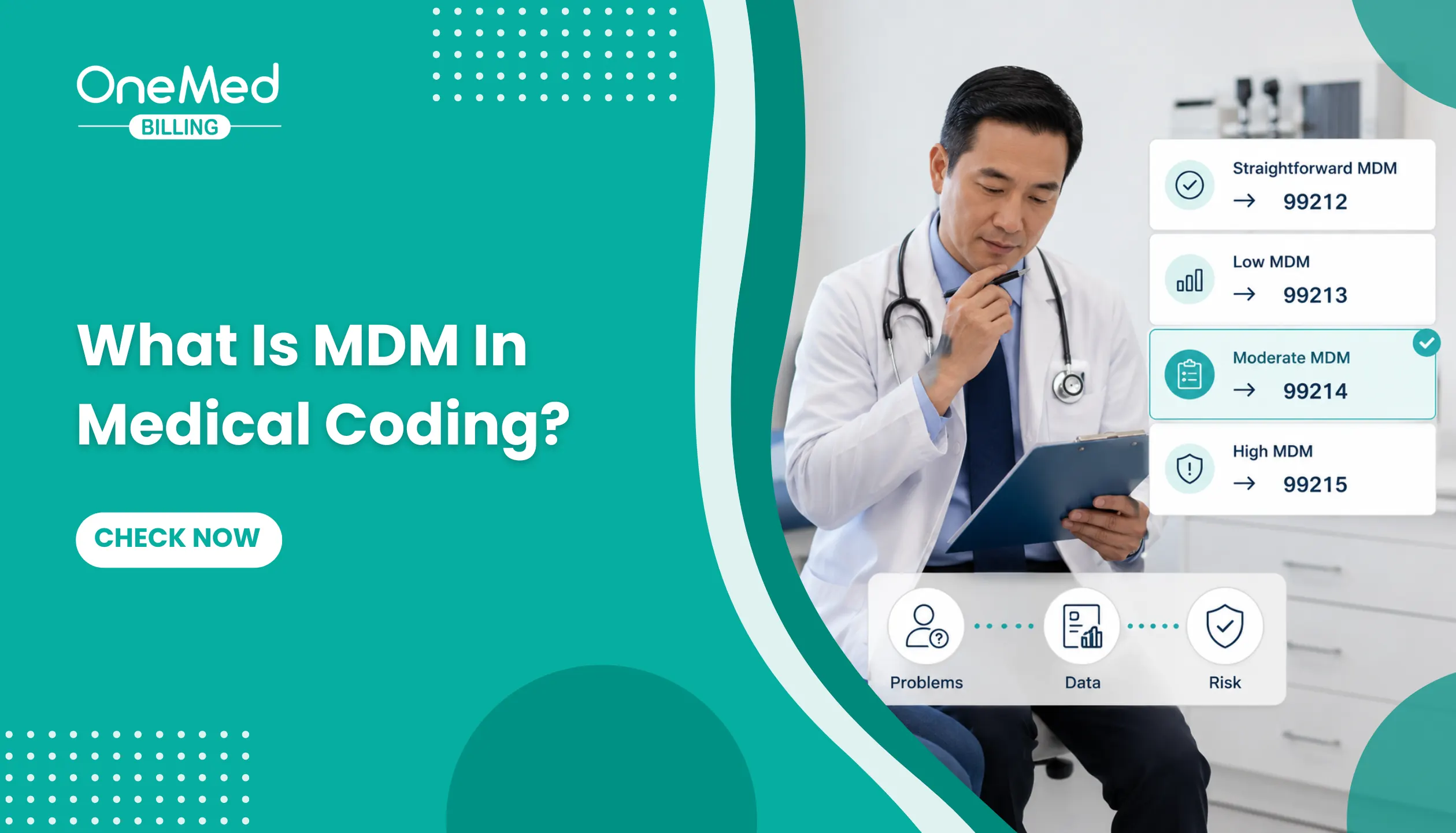
MDM levels help determine which E/M code can be supported for an office or outpatient visit. For established patient visits, the MDM level commonly connects to codes 99212, 99213, 99214, and 99215.
The higher the documented MDM complexity, the higher the E/M code that may be supported. But the selected code must match what the documentation shows. A higher code should not be selected only because the patient has multiple diagnoses or because the visit felt complex.
| MDM Level | Established Patient E/M Code | What It Usually Means |
|---|---|---|
| Straightforward MDM | 99212 | Minimal problem, limited decision-making, low clinical work |
| Low MDM | 99213 | Stable or uncomplicated problem with limited risk |
| Moderate MDM | 99214 | More complex problem, prescription management, higher data review, or increased risk |
| High MDM | 99215 | Serious condition, high-risk decision-making, or significant threat to health |
For example, a routine follow-up for a stable condition may support 99213 if the decision-making is low. A visit involving worsening symptoms, prescription changes, lab review, and documented risk may support 99214 if at least two MDM elements meet the moderate level.
A 99215 usually requires high-complexity MDM. This may involve a serious illness, major treatment risk, intensive monitoring, or a condition that could threaten life or bodily function. The documentation must clearly show why the encounter reached that level.
MDM Examples for Common E/M Codes
The same diagnosis does not always support the same E/M code. The correct code depends on the documented MDM level, including the problems addressed, data reviewed, and risk involved in the visit.
These examples show how different MDM levels may support common established patient E/M codes such as 99212, 99213, 99214, and 99215.
99212: Straightforward MDM Example
A patient comes in for a simple follow-up on a minor skin irritation that is already improving. The provider reviews the condition, confirms there are no new symptoms, and recommends continuing basic care.
This may support 99212 because the problem is minor, there is little or no data reviewed, and the risk is minimal.
99213: Low MDM Example
A patient with stable hypertension comes in for a routine follow-up. The provider reviews the blood pressure reading, confirms the medication is working, and continues the same treatment plan without major changes.
This may support 99213 because the condition is stable and the visit involves low-level decision-making.
99214: Moderate MDM Example
A patient with diabetes comes in with worsening blood sugar readings. The provider reviews recent lab results, adjusts medication, discusses diet and monitoring, and plans follow-up care.
This may support 99214 because the visit includes a chronic condition with worsening control, data review, and prescription drug management.
99215: High MDM Example
A patient presents with severe symptoms that may indicate a serious condition. The provider reviews available test results, considers urgent treatment options, discusses the need for hospital evaluation, and documents the risk involved in the decision.
This may support 99215 because the visit involves high-risk decision-making and a condition that may pose a serious threat to the patient’s health.
The key point is that the E/M code should match the documented MDM level. A visit should not be coded higher only because the patient has multiple diagnoses. The documentation must clearly show what the provider evaluated, reviewed, and managed during that specific encounter.
Common MDM Documentation Errors That Affect E/M Coding
Even when the provider makes the right clinical decision, the E/M code can still be incorrect if the documentation does not clearly support the MDM level. Most MDM errors happen when the chart does not show what was addressed, what was reviewed, or what risk was considered during the encounter.
1. Problem Listed but Not Addressed
A diagnosis on the problem list does not automatically count toward MDM. The provider must show that the problem was evaluated, treated, monitored, or managed during that visit.
For example, if diabetes is listed in the chart but the visit only addressed a sore throat, diabetes should not increase the MDM level unless it was actually addressed.
2. Data Reviewed but Not Documented
If the provider reviewed labs, imaging, outside records, or test results, that review should be documented clearly. If it is not documented, the coder may not be able to count it toward the data element.
For example, writing “labs reviewed” is weaker than documenting which labs were reviewed and how they affected the treatment plan.
3. Risk Not Clearly Explained
Risk must be supported by the provider’s decision-making. If medication is changed, a procedure is considered, hospitalization is discussed, or treatment is limited by patient factors, the documentation should explain that clearly.
For example, simply listing a medication may not be enough. The note should show whether the provider started, adjusted, monitored, or discussed risks related to that medication.
4. MDM Level Chosen from One Element Only
A visit should not be coded based on one MDM element alone. The final MDM level usually requires at least two of the three elements to support the same level.
For example, a serious diagnosis may not support a higher E/M code if there is no matching documentation for data reviewed or risk involved.
5. Time Used When MDM Better Supports the Visit
Some visits may support a stronger E/M level through MDM than through total time. If the provider only documents time without showing the complexity of the problems, data, and risk, the visit may not reflect the full clinical work performed.
How to Improve MDM Documentation and Coding Accuracy?
Improving MDM accuracy starts with making the provider’s decision-making clear in the note. The coder should be able to see what was addressed, what was reviewed, and why the treatment plan supports the selected E/M level.
Simple ways to improve MDM accuracy include:
- Document the problems addressed: Clearly mention which conditions were evaluated, monitored, treated, or changed during the visit.
- Avoid listing inactive diagnoses: Do not count a diagnosis just because it appears in the problem list. It should be addressed during that encounter.
- Record the data reviewed or ordered: Note labs, imaging, outside records, test results, or referrals reviewed or ordered during the visit.
- Explain the risk: Document medication changes, treatment risks, surgery decisions, hospitalization considerations, or other factors that affected the plan.
- Use clear assessment and plan notes: The note should show why the provider chose a specific treatment, follow-up, or management decision.
- Review at least two MDM elements: Before selecting the E/M level, confirm that at least two of the three MDM elements support the code.
- Train providers and coders together: Providers should understand what details coders need, and coders should give feedback when documentation is unclear.
- Audit E/M coding patterns regularly: Review 99213, 99214, and 99215 patterns to find undercoding, overcoding, or documentation gaps.
A consistent MDM review process helps practices choose the right E/M code, reduce coding errors, protect reimbursement, and lower audit risk.
Conclusion
MDM is not just a coding rule. It is the link between the provider’s clinical work and the E/M code submitted on the claim.
For practice owners, this matters because unclear MDM documentation can lead to missed revenue, incorrect coding, denied claims, or audit risk. A visit may involve real clinical complexity, but if the problems addressed, data reviewed, and risk considered are not clearly documented, the code may not be fully supported.
Improving MDM accuracy helps practices bill E/M visits more confidently, reduce undercoding and overcoding, and make sure reimbursement reflects the level of care provided. The best approach is simple: document the decision-making clearly, review all three MDM elements, and choose the E/M code that the record can actually support.
Frequently Asked Questions
Find quick answers to common questions about this topic, explained simply and clearly.
What Are the 4 Levels of MDM?
The four levels of MDM are: Straightforward Low Moderate High These levels show how complex the provider’s medical decision-making was during the patient visit. The higher the c
What Does MDM Mean in Medical Terms?
MDM stands for Medical Decision Making. In medical coding, it refers to the provider’s clinical thinking and decision-making during a patient encounter. MDM helps determine the correct E/M code based on: The problems addressed The data reviewed or analyzed The level of risk involved in the patient’s care
What Are the Three Elements of MDM?
The three elements of MDM are: Number and complexity of problems addressed This looks at the patient conditions the provider evaluated or managed during the visit. Amount and complexity of data reviewed and analyzed This includes labs, imaging, outside records, test results, or discussions with other providers. Risk of complications, morbidity, or mortality This looks at the risk connected to the patient’s condition or treatment decisions. At least two of these three elements usually need to support the same level to determine the final MDM level.
What Are the First 3 Steps to Implement MDM?
The first steps to implement accurate MDM documentation and coding are: Document the problems addressed clearly Providers should clearly show which conditions were evaluated, treated, or monitored during the visit. Record the data reviewed or ordered Labs, imaging, outside records, and test interpretation should be documented properly. Explain the treatment risk and management decisions The note should show why medications were changed, tests were ordered, or treatment decisions were made.
How Many Types of MDM Are Recognized?
MDM is generally recognized in four levels: Straightforward Low Moderate High These levels are used in E/M coding to measure the complexity of the patient encounter and support the correct CPT code selection.